|
Practicing Providers with Prescribing Authority tab |
|
Purpose |
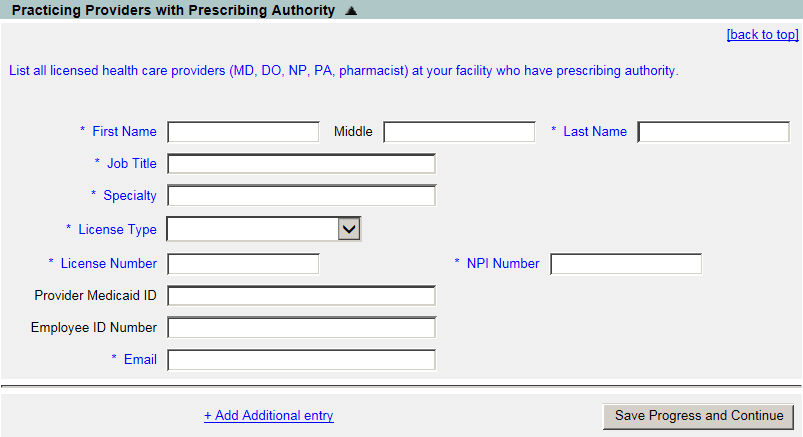
This section captures the practicing provider's information. During a renewal, this information will be prepopulated with the information that was filled in earlier for this organization.
|
Required Fields |
|
Field Name |
Description |
|
First Name |
Required. The provider's first name. |
|
Middle Name |
The provider's middle name. |
|
Last Name |
Required. The provider's last name. |
|
Job Title |
Required. The provider's job title. |
|
Specialty |
Required. The provider's area of specialization. |
|
License Type |
Required. The license type the provider holds. |
|
License Number |
Required. The license number associated to the license type selected. |
|
NPI Number |
Required. The provider's National Provider Index number. |
|
Provider Medicaid ID |
The provider's Medicaid ID. |
|
Employee ID Number |
The provider's employee number. |
|
|
Required. The provider's email address. |
|
+ Add Additional Entry |
Select this to add more providers associated with this organization. |