|
Responsible Medical Provider/Medical Director tab |
|
Purpose |
This accordion tab will be displayed with a different tab header based on the organization category.
|
Required Fields |
|
Field Name |
Description |
|
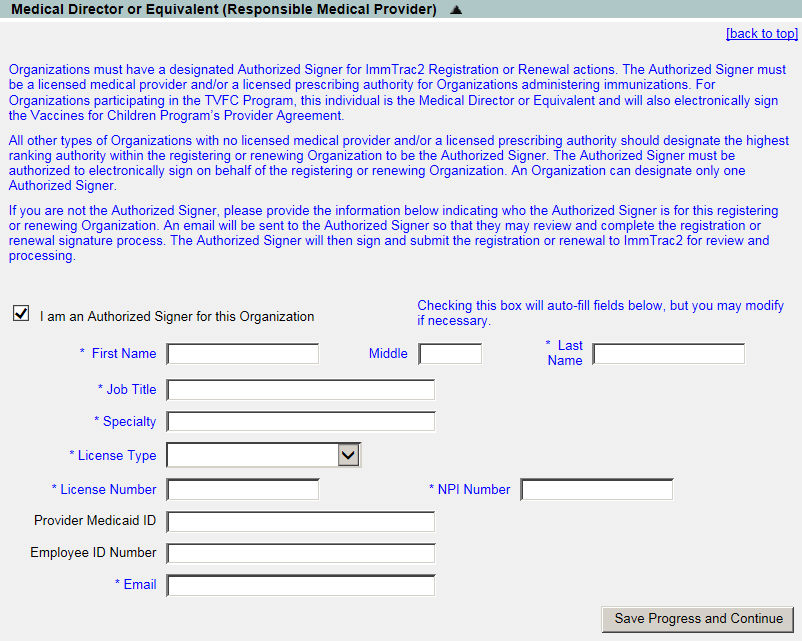
I am an Authorized Signer for this Organization |
If you are the authorized signer for this organization, check the box and the details will be prepopulated with your details. You can modify, if needed. |
|
First Name |
Required. The provider's first name. |
|
Middle Name |
The provider's middle name. |
|
Last Name |
Required. The provider's last name. |
|
Job Title |
Required. The provider's job title. |
|
Specialty |
Required. The provider's area of specialization. |
|
License Type |
Required. The license type the provider holds. |
|
License Number |
Required. The license number associated to the license type selected. |
|
NPI Number |
Required. The provider's National Provider Index number. |
|
Provider Medicaid ID |
The provider's Medicaid ID. |
|
Employee ID Number |
The provider's employee number. |
|
|
Required. The provider's email address. |